The Food and Drug Administration’s job is to protect the public from snake oil and dangerous drugs. But by telling all health care professionals to immediately stop giving the Johnson & Johnson vaccine because of one death in 7 million people, they have transitioned to paternalism. This is not botox, this is a life-saving medication. If the FDA applied their logic to other medications, we would not have antibiotics, Tylenol, or oral contraceptive pills. What ever happened to giving people the data and letting them make their own health decisions?
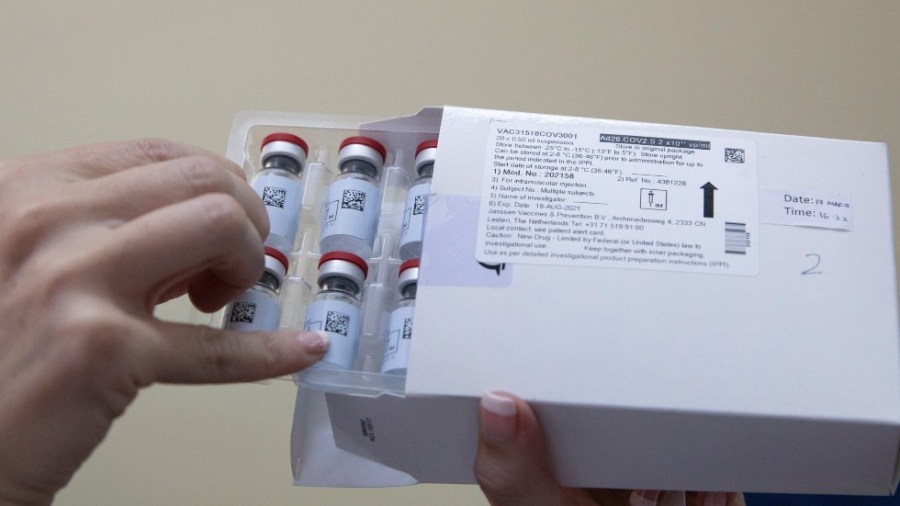
The eight known blood clot complications after the Johnson & Johnson vaccine, including one death, have been observed in people under age 50, all but one were in women. The FDA should have responded by pausing the Johnson & Johnson vaccine in that specific group.
Instead, they effectively halted the Johnson & Johnson vaccine rollout and created messaging whiplash for millions who are not in that risk group. In fact, simultaneous to the Johnson & Johnson news this week was a New York Times headline calling for vaccine mandates. The FDA’s action might be appropriate if we were not in a public health emergency or had more supply than demand. But that was not the case. We have roughly 1 in 670 Americans who have died of coronavirus and approximately one in 7 million people dying from one of the vaccines that prevents it.
The FDA argued that the halt was also to educate doctors not to use heparin to treat these clots, which are seen in the setting of a low platelet count. I’d personally like it if more doctors would prescribe insulin the right way. That doesn’t mean we shut down insulin injections until we can educate doctors on it. Moreover, it’s not rocket science for a doctor to avoid heparin in a patient with a blood clot and very low platelet count — avoiding heparin in that clinical situation is standard of care. The FDA could have simply issued an advisory on how to manage these clots. As editor of one of the two largest trade publications for physicians (MedPage Today), I can assure you that the information would have been disseminated instantly.
To justify the halt for all Americans, the FDA used its eternal excuse of safety. Under the guise of using “abundant caution,” as if doing so is not a tradeoff, they are suggesting that they are siding with less population risk, when they may be increasing population risk. But they rarely talk about the hundreds of Americans that have been dying each day from COVID-19 or the race to vaccinate more non-immune people. Not being able to see the forest from the trees while the vaccine is in short supply explains why the FDA has still not approved the Oxford AstraZeneca vaccine, which the U.K. has used along with other vaccines to successfully deliver a first dose to most of its country, partially reopened earlier this week, and plan for a full reopening this summer.
In my study of the FDA over the years, I would describe them as erratic. In 1995, they approved oxycontin for chronic pain despite any shred of evidence to support it for that indication. Ironically, that approval was overseen by Dr. Janet Woodcock, the current acting director of the FDA who co-announced the Johnson & Johnson vaccine halt.
From the start of the COVID pandemic, the FDA has had missteps. In January 2020, the FDA blocked labs and universities from performing COVID tests, telling one doctor he had to print out his application and mail a physical copy along with a CD-ROM or hard drive of his already submitted electronic application. That resulted in a delay of a precious few weeks.
They also seem to lack urgency at times. After the FDA expert panel voted swiftly and unanimously to approve the Moderna vaccine, the American people had to wait two days for their bureaucratic processes, including, oddly, the CDC also approving it separately, before the final authorization was given the green light. Approximately 5,000 Americans died in those two days. What were they doing, looking for a stapler?
Again, after this week’s joint announcement with the FDA and CDC, the CDC convened their experts two days after their decision to shut down the Johnson & Johnson vaccine. A suggestion for our next health emergency — move faster.
More striking, when pharmacists begged the FDA at the height of the pandemic this winter to let them combine unexpected extra partial doses that were noted in vaccine vials, the FDA said no. According to Inova Hospital, pooling the residual as they wanted to do would have increased the vaccine supply by 10 percent. The FDA is usurping the autonomy of physicians to use their own best clinical judgment.
Doctors make recommendations balancing risks with patients every day. Either we are in a health emergency with a vaccine shortage or we don’t need this life-saving intervention right now. It can’t be both.
The FDA and Centers for Disease Control and Prevention are using peacetime thinking — even more strict than they use to regulate lifestyle medications. But some parts of this country are still at war with this virus. The old guard medical establishment seems uncomfortable recognizing that we have been rationing a life-saving resource. That’s also why they rejected the maximize first dose approach the U.K. used to surpass the U.S. and crush their epidemic (the U.S. has vaccinated 49 percent of adults; the U.K. has vaccinated 62 percent of adults) despite both countries having administered nearly the same amount of vaccines per capita (as of April 15, 59 doses/100 people in the U.S. versus 61 doses/100 people in the U.K.).

We need better medical leadership.
Marty Makary M.D., M.P.H. is a professor at the Johns Hopkins School of Medicine, Bloomberg School of Public Health, and Carey Business School. He is chief medical advisor to Sesame Care and author of the upcoming paperback book The Price We Pay.