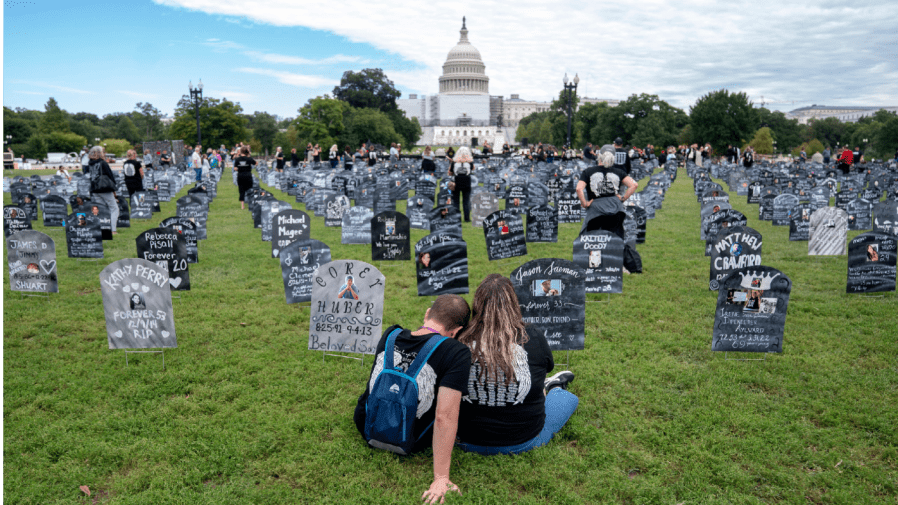
In 2021, more than 100,000 Americans lost their lives due to a drug overdose. America’s overdose epidemic is getting worse, as increasingly lethal substances enter the market.
The reality of overdose and the toll it takes on communities is heartbreaking. Yet even now, there is hope. The U.S. Department of Health and Human Services recognizes the central role recovery plays in reducing overdose deaths. Today, more than 20 million people are in recovery from a substance use disorder, a milestone we mark as we close out the month of September as National Recovery Month.
Recovery Month is also a call to action to create a wider, deeper and more nuanced approach to building healthy communities. We can achieve this in part by creating more robust training in addiction science and policymaking, and by engaging people in recovery in a meaningful way in policymaking.
As the former director and acting director of the White House Office of National Drug Control Policy, we have witnessed firsthand the results of addiction policies based on neither science nor evidence. In spite of this, little has been done to build capacity in addiction policymaking. Georgetown University is one of the first educational institutions to establish a Master of Science in Addiction Policy & Practice, as well as an Addiction Policy Scholars program. These efforts seek to build the addiction policy workforce with the end goal of improving our nation’s drug policies.
The working definition of recovery is, “a process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.” Good health, a stable home, a supportive community and a sense of purpose are all dimensions of living a full life in recovery. Yet barriers to health care, housing, employment and education — often the result of a punitive or moralistic response to addiction — stand in the way of this goal.
Removing these barriers and the stigma that accompanies them are central to any policy solution to address overdose rates, overdoses that have hit Black and Native American communities especially hard. Individual and culturally competent recovery supports and policies must address the drivers of addiction, drivers that include intergenerational trauma.
For decades, many of the nation’s addiction policies have been rooted in fear and stigma, not science and compassion. In both the Biden and Obama administrations, where both of us served, we began to make headway by changing how we talk about people with substance use disorder and increasing access to evidence-based treatment and harm reduction services. However, even these steps have not met the urgency of the moment.
Limited access to treatment with buprenorphine or methadone, the “gold standard” of care for opioid use disorder, persists. For example, before a person can receive methadone treatment for an opioid use disorder, they must have an opioid use disorder for a year. The stringent regulatory regime for methadone has developed over time with the primary goal of controlling access to life-saving medication, rather than providing care to people in need.
A widely accepted tenet of the recovery movement is that there are many roads to recovery. Nevertheless, the nation’s approach to addiction is built on laws and regulations that assume every person is the same and that what worked for one person works for everyone. Furthermore, if a person returns to the use of alcohol or other drugs, a common occurrence during the treatment process, they may be ordered to a jail cell, when what is needed is a therapeutic approach.
It is unthinkable to apply this logic to cancer treatment, diabetes or other chronic health conditions.
Changing course in addiction policymaking will not happen overnight. Investing in the addiction policy workforce is long overdue and necessary to make the bold choices needed to improve the lives of people and communities affected by addiction.
Michael Botticelli served as director of National Drug Control Policy in the Obama administration. The U.S. Senate unanimously confirmed him in 2015. Regina LaBelle is a distinguished scholar and director of the Addiction and Public Policy Initiative at the Georgetown University Law Center’s O’Neill Institute. She served as acting director of National Drug Control Policy in the Biden administration in 2021.