A better way to rein in Medicaid


Medicaid is two things at once: a health care benefit for poor individuals, and a system of federal grants that disproportionately profits wealthy states.
Over the past four decades, Medicaid spending has grown more than any other category of public expenditure. Republicans have tried to rein in the cost of the program with “block grants” and “per capita caps.” But these would leave states short of funds in recessions, threatening state budgets and coverage for low-income beneficiaries when assistance is most needed. As a result, Congress has repeatedly rejected these proposals — even under unified GOP control.
A better approach would be to gradually federalize responsibility for covering individuals that states must enroll in Medicaid, while leaving states to pay for whatever additional benefits they choose to provide out of their own funds.
Medicaid has been the fastest growing government program over recent years, expanding from 0.5 percent of gross domestic product in 1985 to 2.4 percent of GDP in 2022. This is partly due to the general increase in health care costs, but mostly the product of substantial expansions in eligibility. Medicare’s enrollment surged from 20 million in 1985 to 86 million in 2021 — an increase from 8 percent to 26 percent of the U.S. population.
Over that period, the expansion of Medicaid contributed to a decline from 15 percent to 11 percent in the proportion of the U.S. population that lacks health insurance. But one study estimated that for 60 percent of those newly enrolled, expansions of Medicaid coverage had simply served to displace private insurance.
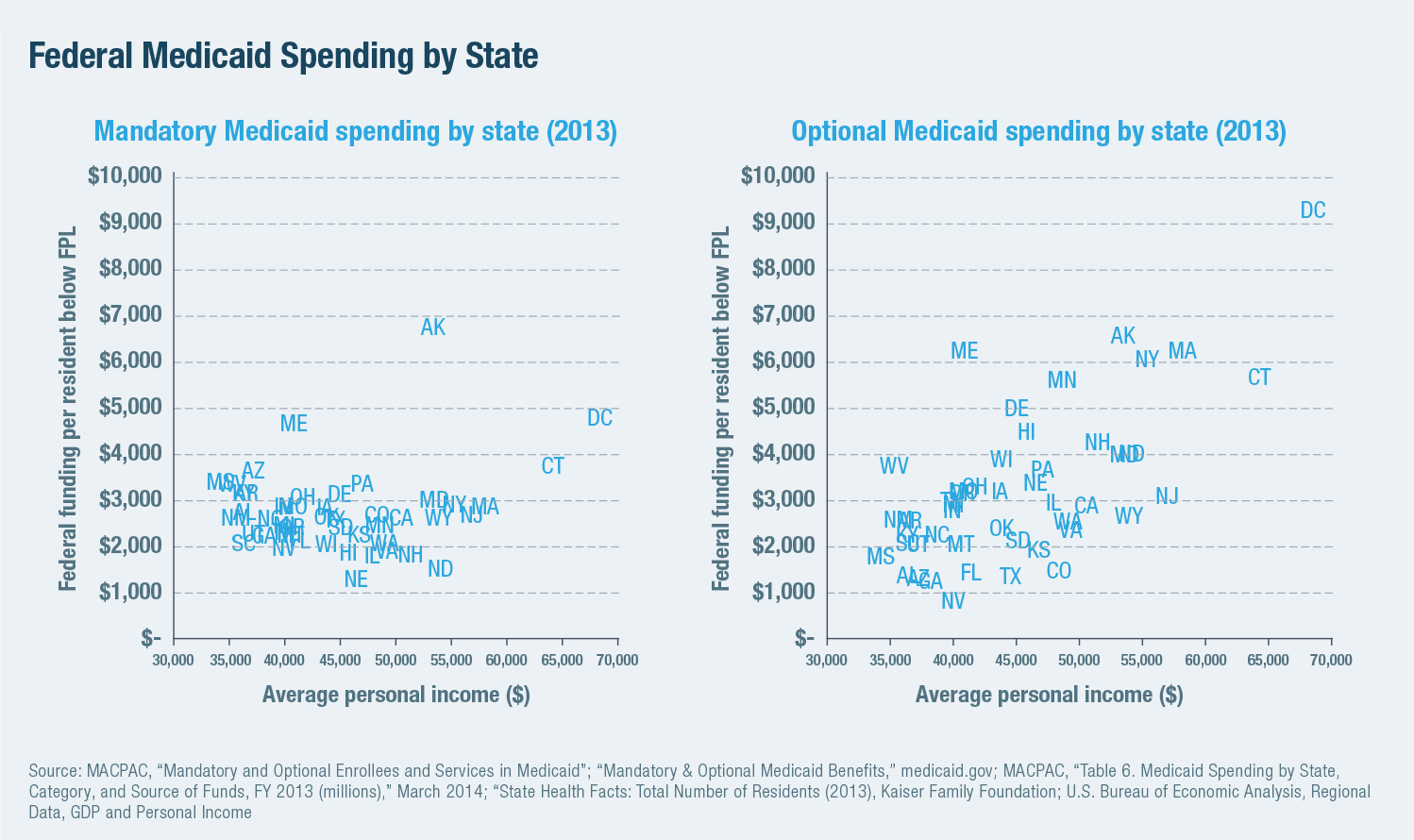
Medicaid is largely structured and operated by states, with funding mostly provided by the federal government. States can claim between $1 and $9 in federal funds for every $1 they spend on the program for eligible beneficiaries, which gives them a great incentive to expand the program as much as they can. The wealthiest states with the deepest tax bases have been most able to take advantage of this arrangement: Alaska claimed $21,445 in federal Medicaid funding per resident in poverty in 2021, whereas Nevada received only $8,402. During economic expansions, states have used growing revenues to expand Medicaid, and repeatedly prodded Congress to bail them out in subsequent recessions.
For decades, congressional Republicans have sought to rein in Medicaid costs by capping federal matching aid each state can claim for each beneficiary. (This was how grants to states under the Social Security Act were all initially structured.) But this proposal has repeatedly run into a combination of substantive objections and political obstacles, which are unlikely to disappear.
Opponents have argued that capping Medicaid grants to states would threaten the funding of health care for the neediest beneficiaries. This problem would be particularly acute in recessions, when state tax revenues decline just as their Medicaid caseloads increase — exacerbating the bailout dynamic. It would also leave states in a bind if medical costs suddenly surged beyond their fiscal capacities. As proposed caps have been based on historical spending, traditionally low-spending states would have become subject to the tightest constraints. This has made per capita caps unpopular with many Republican governors as well as Democrats.
To meet these objections, the proposed caps considered (and rejected) by the Republican Congress in 2017 were so watered down that they would have been entirely ineffectual. They would have limited the growth of federal Medicaid grants to 3.7 percent per enrollee per year, even though spending had only grown at 2.0 percent per year over the previous 16 years. Nor would per enrollee caps have done anything to constrain the cost of expanding enrollment, which is the main driver of rising expenditure.
Reformers would achieve more by distributing Medicaid funds according to the needs of individuals, rather than in proportion to the resources that states are able to contribute.
To claim federal Medicaid funds, states are currently required to cover a core package of services (hospital, physician and nursing home care) for groups of mandatory beneficiaries (such as pregnant women, the disabled and children with incomes below the poverty line). They may also claim federal funds at the same matching rate to provide additional services (such as optical or dental care) and for expanding eligibility to individuals with incomes up to 380 percent of the federal poverty line.
Across the country, federal payments to states amount to 125 percent of the cost of mandatory Medicaid spending. But while federal assistance for mandatory Medicaid spending is fairly uniform across states, the wealthiest states claim several times more than the poorest in grants for optional benefits. Whereas Nevada in 2013 received federal payments covering 85 percent of the cost of benefits it was required to provide, the District of Columbia was able to claim 203 percent.
The core problem with Medicaid is the separation between control over the cost of the program (the scope of benefits, fees paid for them and the breadth of eligibility) and the responsibility for paying for it. Ideally, the federal government should directly operate and fully fund mandatory Medicaid benefits, and let states fully fund any additional benefits they choose to provide out of their own resources.
Such an arrangement would represent a big change from the status quo; thus, a more incremental reform path to get there is necessary.
To achieve this, federal payments to each state should be capped at either (1) 100 percent of the cost of providing core benefits to mandatory enrollees, or (2) the current per resident level of federal funding in nominal terms — whichever is higher. States should be allowed waivers to claim federal funds at a higher matching rate to fund mandatory spending by reducing federal aid claimed for optional spending by an equivalent amount.

This reform would focus federal Medicaid spending on the provision of core benefits for the neediest enrollees. Rather than leaving states short of funds in recessions when program costs increase, it would make the federal government largely responsible for costs resulting from increased enrollment among core eligibility groups in such circumstances.
Yet, such a reform would eliminate the incentive for states to expand the cost of Medicaid at the expense of the federal government. Over time, it would reduce real federal Medicaid spending by 20 percent, as inflation erodes the real value of grants to states where spending on optional benefits exceeds the full cost of mandatory spending. The reduction in federal spending would be limited to optional benefits and concentrated on the wealthiest states. By harmonizing benefits and reducing the disparity in assistance to states over time, this would facilitate the eventual full federalization of the program.
Chris Pope is a senior fellow at the Manhattan Institute.
Copyright 2023 Nexstar Media Inc. All rights reserved. This material may not be published, broadcast, rewritten, or redistributed. Regular the hill posts




{kind=link}
The Hill Podcasts


